
HCC CODING
Hierarchical condition category (HCC) coding is a risk-adjustment model originally designed to estimate future health care costs for patients. The Centers for Medicare & Medicaid Services (CMS) HCC model was initiated in 2004 and is becoming increasingly prevalent as the environment shifts to value-based payment models.
HCC coding relies on ICD-10-CM coding to assign risk scores to patients. Each HCC is mapped to an ICD-10-CM code. Along with demographic factors such as age and gender, insurance companies use HCC coding to assign patients a risk adjustment factor (RAF) score. Using algorithms, insurance companies can use a patient’s RAF score to predict costs. For example, a patient with few serious health conditions could be expected to have average medical costs for a given time. However, a patient with multiple chronic conditions would be expected to have higher health care utilization and costs.
HCC coding helps communicate patient complexity and paint a picture of the whole patient. In addition to helping predict health care resource utilization, RAF scores are used to risk adjust quality and cost metrics. By accounting for differences in patient complexity, quality and cost performance can be more appropriately measured.
Prospective Review
A prospective coding review process is intended to help physicians prepare for upcoming patient encounters. Reviewers—who are often certified risk coders—evaluate the patient’s HCC code history, prescription drugs, hospital records, lab results, and physician notes. They may also leverage access to out-of-network claims, which helps establish a 360° view of available clinical information. As coders review the medical record, they identify patients with likely HCC conditions whose diagnosis codes have not been captured accurately. Once the HCC opportunity has been identified, the next step is to prepare the physicians to address the condition(s) at the upcoming appointment. This communication is often performed via updates to the EHR problem list or delivered to the physician ahead of the patient’s visit via a morning huddle or similar type of meeting. The physician must then ensure that the noted conditions are documented and included in the encounter as appropriate. If the physician’s examination of the patient supports the HCC condition, he or she will then document and capture the HCC code(s) during the encounter. Employing staff members, who assist with pre-visit planning, significantly improves the process and reduces the burden put on the physician.
Concurrent Review
In a concurrent coding review process, coders review the EHR/medical notes and HCC codes in real time before the claims are submitted to payers. In many cases, coders will leverage existing EHR and RCM technology to enable this type of review. (Note: most organizations leverage claim scrubbers or similar technology to review fee-for-service claims before they are submitted to payers.) This process helps ensure the diagnosis coding accurately supports what the physician documented in the EMR. In many cases, the physician will perform robust clinical documentation but may not select the most appropriate ICD-10 code. Having the medical coding team perform this concurrent review prior to claim submission achieves two benefits. First, it ensures the physician's hard work in delivering and documenting care is correctly translated into accurate HCC codes. Second, it ensures the payers have the correct HCC codes on the initial claim, eliminating the need for an additional retrospective review. Concurrent review works best in tandem with other initiatives such as prospective review and physician education.
Retrospective Review
Retrospective coding review occurs after care has been delivered and claims have been submitted to the payer. Such reviews often uncover HCC codes supported by the medical record that were not reported, as well as HCC codes that should not have been submitted because they did not meet documentation guidelines.
Because the retrospective approach reviews charts later rather than in real time, clinical documentation issues identified are likely to be longstanding ones. It also requires a secondary process to flag the charts and send the corrected HCC coding information to the payer. This process is often used with Medicare Advantage programs, which have a relatively straightforward method for submitting retrospective coding adjustments known as the Alternate Submission Method (ASM). This process becomes more difficult in ACOs and CPC+ programs where submitting retrospective coding adjustments is cumbersome.
Type of records
we Code
-
History and Physical Reports (Out Patient)
-
Progress Notes (Out Patient)
-
Consultations (Out Patient)
-
Consultation Letters (Out Patient)
-
History and Physical Reports (OP & In Patient)
-
Discharge Summary Reports (In Patient)
-
Consultation Reports (OP & In Patient)
We Don't Code
-
Lab Visits
-
Progress Notes (In Patient)
-
Patient Assessment Forms.
-
Notes on Telephone Calls & Messages.
-
Letters from Physician to Patient.
-
Letters from Patient to Physician.
-
PT/INR, Immunization or Injection visits.
-
Encounters that are not determined as face-to-face
Our team consists of experienced and certified CCS and CCA professionals from AHIMA (American Health Information Management Association) and also certified CPC, COC & CIC professionals from AAPC (American Academy of Professional Coders) who are continuous with the US healthcare knowledge and talent attending online seminars and maintaining their credentials through CEU’s (Continuing Education Units).
We focus and execute strong maturity on maintaining the best quality standards across the organization. We adopt the latest practices and best methodologies with an uncompromising approach warranting excellence in delivery.
Our Strengths
Regular Audits
During Regular Audit/Focus Audit Process, we classify the QA into types of errors, including, known errors, conceptual errors, repeated errors, and typographical errors. Based on the type of errors, we will provide retraining for the conders and then ensure all coders are on same page
Continuing Education
Sometimes, when coder(s) miss the guidelines/client specifications, we conduct daily refresher training and weekly coder calibration tests, etc
See-Saw Audits
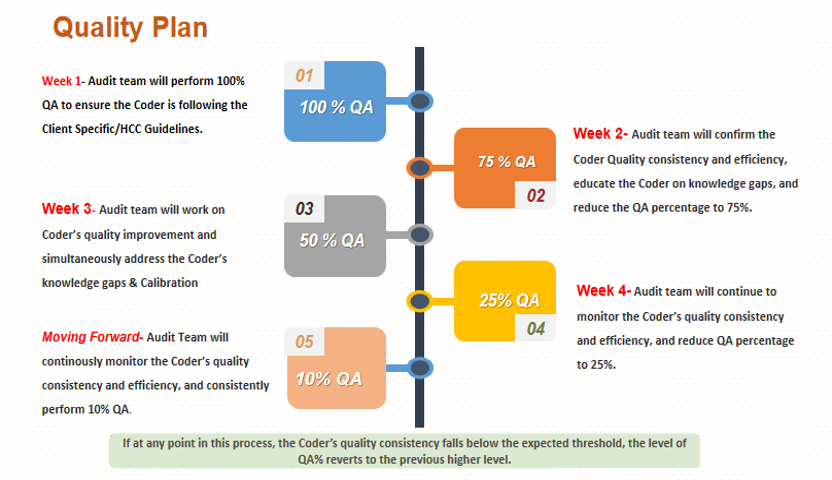
For every three months we perform see-saw audit where we will increase the audit percentage from 10% to 100% and will gradually come back to 10% to ensure all the coders are consistent in quality and up to date in guidelines.


The first step is to check for the
Primary Identifier (Patient Name)
&
Secondary Identifier (Date of Birth, SSN# or MRN# )
in the Entire Medical Record in order to confirm
that the Medical Record belongs to that particular patient.
-
To consider a note as complete and face-to-face it should have minimum requirements like subjective(reason for visit ), vital signs, physical exam, review of systems, assessment and plan.
-
If a note does not contain the minimum requirements it is considered as an incomplete note and is not legible to code.
-
-
Diagnoses listed in Assessment with support
-
Diagnoses in Plan with support
-
Diagnoses in HPI/Subjective/Chief Complaint with support
-
Diagnoses in Review of Systems with support
-
Diagnoses in Past Medical History with support
-
Diagnoses in Physical Exam without any support.
-
Any disease condition should be supported with a drug or plan as to ensure that the patient is on current treatment or getting treatment in future and/or satisfy the MEAT concept
-
Monitoring,
-
Evaluating,
-
Assessment
-
Treatment
(OR) Any disease condition should be supported with a drug or plan as to ensure that the patient is on current treatment or getting treatment in future and/or satisfy the TAMPER concept-
Treatment
-
Assessment
-
Monitor/Medicare
-
Plan
-
Evaluate
-
Referral
-
There are 11,523 Hcc and RxHcc Mapping ICD 10 Codes for the Mid Year 2023
-
Legible patient name (*First, Middle, *Last Name).
-
Secondary Identifier (DOB, SSN#, MRN#).
-
Legible Date of Service.
-
Legible Signature (Credential & date) that meets CMS Guidelines.
-
-
All the dates of service that are identified for review must be signed (with credentials) and dated by the physician or an appropriate physician extender (e.g., nurse practitioner).
-
The physician must authenticate each note for which services were provided.
-
Acceptable physician authentication comes in the forms of handwritten signatures and electronic signature.
-
A legible electronic signature should contain proper verbiage or authentication statement, date of signature and proper positioning of the signature at the end of the document.
-
Our team of professionals

Dr. Talya Sulami
Head of clinic

Dr. Tom Chie
Family doctor

George Mekler
Therapist

Elinor Jonas
Speech therapist

Lee Levin
Hospice nurse

Shaya Raviv
Nutritionist
What our patients are saying
This is the space to share a review from one of the business's clients or customers.
Eden Rachim
This is the space to share a review from one of the business's clients or customers.
Naya Denner
This is the space to share a review from one of the business's clients or customers.
Lenny Yliuay